Dr. Nick Doyle, O.D., talks about Keratoconus and various eye conditions that can be helped with specialty contact lenses.
KERATOCONUS & SPECIALTY LENSES
Hi everybody! This is Dr. Nick Doyle from Highline Vision Center and I’m one of the four optometrists here. I just wanted to take an opportunity to talk to you today a little bit about one of my passions and areas of expertise within the practice, which is seeing patients who have Keratoconus and specifically fitting those patients with specialty contact lenses.
TYPES OF REFRACTIVE ERROR
To understand a little bit about what we’re talking about in the first place, it’s helpful to talk a little bit about different types of what we call refractive error, or what you may know as your prescription for glasses or contact lenses, and up here we’ve listed the four different, main types of refractive error:
- Myopia
- Hyperopia
- Astigmatism
- Presbyopia
The most two common being myopia and hyperopia which we know as nearsightedness and farsightedness, and then astigmatism and then presbyopia. And presbyopia is simply the type of refractive error that we start to see around 38 to 42 years old when the lens inside the eye gets a little bit less flexible, and that’s when our patients start to need reading glasses or bifocals or even progressive lenses.
ASTIGMATISM
I’m going to touch a little bit more on astigmatism correction because I think astigmatism sometimes gets just a little bit of a bad rap because it sounds different than nearsightedness or farsightedness, and astigmatism really is when the cornea, or the front surface of the eye, is more curved in one direction than another, it’s not totally spherical, and so the common example that we’ll use, that’s a little bit extreme but it helps to get the point across, is your eye is the shape of a football rather than the shape of a baseball.
TOPOGRAPHY
One of the instruments that we will be talking about a little bit in regards to diagnosis, not only of keratoconus but astigmatism, is a corneal topographer. And, a corneal topographer takes a detailed image of the front surface of your eye or your cornea, and it helps us to really easily visualize those curvature changes on the cornea. This [see graphic at 2:23] happens to be a topography map of a patient who has absolutely no astigmatism correction. You’ll see there’s a uniform color here on the map on the right; it looks pretty uniform yellow, and we’ll contrast that with a patient who has what we call “with the rule” astigmatism [see graphic at 2:52]. And, you’ll very readily see that this particular image has what we call a characteristic hourglass shape where you see what we call these hotter colors, your reds, kind of pinks, and oranges concentrated into this figure eight or hourglass shape, and that just indicates that this patient’s cornea is more curved in this direction. So, this is a patient who has what we call regular, “with the rule” astigmatism and we can use glasses and contacts to correct for that.
CORNEAL ECTASIA
We’re going to get into talking a little bit about keratoconus at this point, and keratoconus is a type of what we call a corneal ectasia. As many medical terms do, ectasia comes from a Greek word ectasis, which means stretching, and so we’ll get into that a little bit, but keratoconus, or the corneal ectasias in general, are types of corneal diseases that cause progressive thinning and steepening or that stretching of the front surface of your eye. When you talk about the cornea, in general, it’s about the thickness of a credit card, give or take a little bit, so you can imagine what stretching something that thin, that accounts for about two-thirds of the light bending power of your eye, in general, can do to your vision. But, there’s some basic, different types of ectasias that we deal with in the office, keratoconus being the main one.
There’s a slight variation of keratoconus that we call marginal degeneration keratoglobus, which is a much more severe form of keratoconus, and then we can sometimes see these corneal ectasias in patients who’ve undergone refractive surgeries such as RK (radial keratotomy), PRK, and lasik, potentially if they had too much surgery for what their corneas could handle. Thankfully, we don’t see this often because most of the refractive surgery offices in the area, especially the ones we send our patients to, do a very good job of screening patients to make sure they don’t have any underlying corneal conditions that could cause this.
KERATOCONUS
If we get into talking a little bit more specifically about keratoconus, because that’s what the majority of this presentation deals with, it sounds like it’s rare because the numbers would tell us that, really, it’s about 50 to 230 people per
100,000 in the population, it’s actually quite common. I see keratoconus easily on a weekly basis, depends on the week – sometimes on a daily basis. Usually the onset of this, even though it may not be detected at this time, is before puberty. Sometimes keratoconus will progress through your early forties, and it really depends on a lot of different genetic factors, but it typically affects both sexes, men and women equally.

There are genetic factors that are at play here, and, again, we’ll talk a little bit more about that because that’s an opportunity that we have now available to us to detect this thing a little bit earlier. Some patients have some specific enzyme abnormalities that can cause this to happen; there are certain rare connective tissue disorders that can cause this to happen. We talked a little bit about refractive surgery, things like lasik being at play here, but I want to touch specifically on two of the more common things that we will see, and that is patients who have chronic allergies and do a lot of eye rubbing. And we’re not just talking about eye rubbing occasionally, we’re talking about people who are really rubbing their eyes constantly because they’re always itching.
Keratoconus is a progressive disease, remember we talked about that stretching, but it causes progressive steepening or more curvature to the cornea and thinning of that cornea. Remember, that cornea is pretty thin already. We talked about it being about the thickness of a credit card. The younger that you are when you develop keratoconus, the faster that it progresses, and we can kind of use that a little bit to our advantage in some of the treatments that are available. We’ll get into that a little bit later.
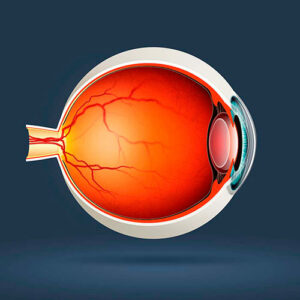
This is a profile image of someone’s eye who has keratoconus. You can see that it’s starting to form kind of a cone shape on the front surface here because the front surface of that eye is starting to get a little bit thinner; it’s starting to become more curved or stretched.
IRREGULAR CORNEAL ASTIGMATISM
And so, if we contrast this topography map of a patient who has keratoconus with the one that we saw earlier that was kind of that nice regular figure eight or hourglass type shape, you’ll notice that there’s still that hot spot of colors here where the cornea is more curved, but that spot up here is missing, and that’s because keratoconus causes very irregular or asymmetrical astigmatism correction. This gets very difficult sometimes for us to correct with standard glasses because it’s almost like the front surface of the eye is warped, and so no matter what we do with a lens and a pair of glasses, that light passes through the lens and the glasses, the glasses bend the light as they’re supposed to do to – try to correct the prescription – and then that light hits this warped surface again and it kind of scatters everywhere. We do have ways to deal with this.
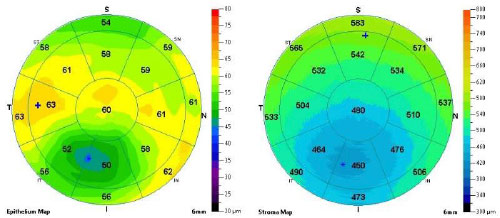
PACHYMETRY
This is a similar patient with keratoconus, it’s what we call a pachymetry map. The pachymetry map helps us to measure the thickness of the front surface of the eye. Remember we talked about keratoconus also causing thinning of the front surface, and so you can see right down here where that highly curved area is, you’ll see that these thickness numbers, which are measured in microns, are much thinner than they are in this top surface of the cornea. Again, pretty irregular; it’s not very uniform.
IMPACT ON VISION
And so, you can imagine the impact this has. And, this could be for someone, even what they see when they’re fully corrected with glasses and have keratoconus. Again, because glasses in some patients with keratoconus just aren’t all that effective, but people will often report a lot of halos around lights at night, they’ll report things like streaks through lights, and we’re going to talk a little bit about how we treat these types of things and get these people seeing better.
TREATMENT
The first step, at least in our office, in my patients, the first step is really to talk to patients about eye rubbing. We talked about that being a big risk factor for keratoconus, but we need to stop eye rubbing immediately because there’s some anecdotal case studies that tell us that patients who stop eye rubbing, there’s a significant reduction in the progression, and to help with that, we’ll also start treating patients for any allergies they might have using antihistamine drops, steroid drops, things of that nature.
There’s some other treatments for keratoconus, some of them relatively new – one of them is CXL, stands for corneal collagen cross linking. So, we’ll talk a little bit about what that is, talk about some methods for improving your vision if you have keratoconus. The end stage as far as keratoconus, if it progresses too quickly or too much for us to be able to correct your vision anymore with these other methods would be corneal transplantation, and we do have a fair amount of patients we see still who have had corneal transplants, although it’s a fairly invasive surgery, usually we can get them seeing better with contact lenses and things of that nature after surgery.
COLLAGEN CROSSLINKING: CXL
Collagen crosslinking is a surgical procedure. There are a number of corneal specialists in the area who we refer patients to to have this done. You see on the left we kind of compare cross-linking to having a gel nail done, and I know that sounds kind of silly, but the process is kind of similar in the sense that we’re essentially hardening a resin or hardening something using a chemical reaction that involves UV light.
So, the eye on the right is a patient that’s having cross-linking done. What they do when they do a cross-linking procedure is they essentially are putting riboflavin drops on the surface of the eye and exposing it to certain wavelengths of light, and the cornea is made up of a collagen beam structure, a collagen network, that gives it its strength, the reaction between the light and the riboflavin causes that collagen to become very tightly knit and artificially hardened. And so, what we’re doing is essentially aging the eye on purpose. The collagen in our body actually starts to cross-link itself after we’re 40 years old anyway, which is why we talked about keratoconus progressing through your 40s. It tends to naturally slow down because of this, but we can artificially make that happen and slow the progression through this procedure. And this is something that’s relatively new within the last five or ten years. It’s very safe when done in the right hands, but it’s something that can really stop the progression. It can’t reverse the damage that’s already done but it certainly helps us out in the long run.
SCLERAL LENSES
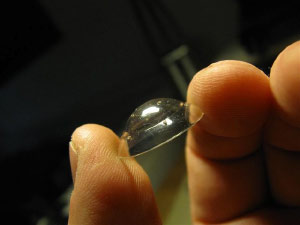
The treatment modality that I’m very passionate about and that I work with frequently is a type of contact lens that’s called a scleral lens, and you’ll see someone holding one of them right here. It’s a very large, or larger than normal, gas permeable or hard contact lens. These are custom made lenses. In many patients, when we show them this lens for the first time they think it’s going to be uncomfortable, but actually, the exact opposite is true. This lens, and we’ll see this in a minute, doesn’t actually touch your cornea. It doesn’t rest on your cornea at all; it fits on the white part of your eye, which makes it very comfortable, and it also means that we’re able to get a contact lens onto the surface of the eye to get the patient seeing better without it continually rubbing over that cone or that area of keratoconus and steepening on the front surface of the eyes. Ultimately it’s a little bit healthier option long-term for these patients to avoid scarring.
WHY DO THEY WORK?
So why does this work better than say a pair of glasses? Well, these contact lens, remember we talked about the patient who has keratoconus having an eye, or front surface of the eye rather, that’s a little bit warped, and so this kind of contact lens actually allows us to create a perfectly smooth, spherical surface on the front of the eye. It’s kind of like we’re temporarily putting an artificially perfect cornea over the one that’s warped, so it allows light to really pass through that lens and create a clear image. Oftentimes, I will see patients who are 20/80, 20/100, even 20/150 out of glasses, and we can get them to see 20/20 out of a scleral lens.
FITTING SCLERALS
From the side, this is what a scleral lens looks like. The lens rests on the white part of the eye, it vaults over the cornea here. There’s space in between the back surface of the lens and the cornea, which we can also see on this OCT scan. This is an instrument we use to help us to fit these lenses, and in doing that, again, we’re not rubbing on the cornea, we’re not creating scarring long term, but we’re getting the patient better vision. This is the same view, or a slightly different view rather, using the same instrument, the OCT instrument, showing where the lens lands on the sclera, or the white part of the eye. Here you can see this transition line here between the sclera and where the cornea actually starts.
OTHER USES FOR SCLERAL LENSES
Scleral lenses are very useful to us for patients with corneal ectasias and keratoconus, but they’re actually useful for multiple different applications. They can be useful for patients who have very severe dry eye, that’s because when you put these lenses in, you actually fill the lens with saline, and so that saline stays between the back surface of the contact lens and the front surface of the eye all day long until you take the lens out, and so for patients with a very severe dry eye that we can’t treat by other means, this is an option because it kind of creates a sealed environment for that patient where their cornea is just bathed in saline solution all day long.
We can use these lenses in patients who have had corneal scarring either due to previous surgery or some type of injury; we use them, as we talked about, in patients who had corneal transplants, and some of them are even useful in patients who have higher prescriptions or patients who need a multifocal type of lens that helps them to see up close and far away; that have higher amounts of astigmatism, and they’re useful for that because some of the lenses, soft lenses, that we use for this just don’t come in parameters high enough to help these patients.
INSERTION, REMOVAL, AND CARE OF LENSES
These are multiple applications for these lenses. They’re a little bit different to put in than a soft contact lens; they require a different technique, which obviously, we teach all of our patients how to do this safely and efficiently, but they require a special insertion and removable devices. They require the patient to fill the lens with saline before they put it in, but the solutions for, as far as cleaning, the lenses are very similar to your standard soft lens solutions, in the sense that we can get what we call multi-purpose solutions, kind of an all-in-one type of storage and cleaning solution. So yes, they take a little bit of getting used to, a little bit of retraining, but we find that most people readily adapt to doing this without any issues.

INSURANCE
We talked about scleral contact lenses being more of a custom option, which sounds a little more expensive, and yes it can be, but insurance often covers these, and vision benefit plans often will cover these under a visually necessary or medically necessary rider on the patient’s plan, and so we do help patients all the time to work with their insurance to make sure that we get the best coverage for these lenses, and obviously we go over all of these costs associated before we even start fitting these contact lenses, but, oftentimes, we can get these lenses almost fully covered by patient’s vision plans, which is nice for those patients who really do need them.
SUPPORTING LOCAL BUSINESS
This is an image of how these lenses are cut; they come from a button of plastic, which is a special type of plastic that’s used to make contact lenses. It’s very breathable. They put the lens on a lathe, and a computer controls how this lens is cut. This is actually an image from a laboratory in Lakewood. The laboratory is called Advanced Vision Technologies; we’ve been using them for all of our gas permeable lenses for a number of years. Now, they do a great job. They’re a locally owned business, which is fantastic, and they have their own designs, which is awesome, because they’re constantly innovating and developing new designs. We’re lucky to have them right in our backyard because they actually ship lenses all over the world.
THE FUTURE
What is the future of keratoconus? What’s the future of scleral contact lens fitting? What technologies are coming down the pipeline here to help us and help patients who have keratoconus? This is the process of something that we call the EyePrintPro lens, which is something that’s now available. The EyePrintPro is very interesting, you may wonder what this blue goo is. I’ve actually had this done on my eye to see what it was like. It’s not painful at all, but the blue goo is a dental impression material that’s been FDA approved for the front surface of the eye, and it helps the contact lens practitioner to be able to take an exact mold of the patient’s eye, who has a keratoconus, and in some patients, who we just can’t get a standard scleral contact lens to work for, this is extremely helpful because we would send this impression back to the laboratory, they can scan it, and they can essentially 3d print a lens that’s custom made exactly for that patient’s eye. Super useful technology; pretty new over the last five years. It’s gaining more and more popularity, but we’re pretty excited that this is something that’s available to us at this point.
On the diagnostic side, this is a genetic test that we can now use called Avigen. Avigen tests, it’s just a cheek swab, so painless, but it tests for 75 genes and over 2000 variations of those genes that influence keratoconus, and so we get a very detailed report back after sending this test into the lab, and we can essentially tell a patient what their risk for developing keratoconus is. Why does this become useful? This becomes useful especially in our patients who, maybe they have keratoconus and we see their children for exams, and we’re starting to see some astigmatism correction, but their topography map is slightly suspicious, but we don’t really know, and so we can do this test very easily with them, find out what their risk is, and potentially monitor them a little more closely, so that if they start to change at all we can get them in right away for cross-linking, so that, hopefully, we don’t end up in a spot where we even need scleral lenses or potentially a corneal transplant down the road.
We can treat this patient for allergies and talk to them about allergies, eye rubbing, sooner to avoid any issues down the road. This is something, that for me, is super exciting because it’s going to allow us to know what’s going on faster than we ever have before.
QUESTIONS?
So that’s about all for today’s presentation, so hopefully that was informative. It’s something that I really enjoy doing. I really enjoy seeing patients in the office and helping them with issues like this, but if you have any questions at all regarding either this presentation or you might have keratoconus or know someone who has keratoconus, please have them call us at the office, the number is listed below.
We’re happy to talk to you about this and happy to do anything we can to help you.
Have a great day!
Ready to Schedule An Appointment?
The Highline Vision Center team is looking forward to seeing you soon. Our practice utilizes state-of-the-art technology to deliver personal and comprehensive eye care for your entire family.